Is Psychiatry Facing an Existential Crisis? Is the title of an article just published on Psychology Today. It’s a book review of Desperate Remedies: Psychiatry’s Turbulent Quest to Cure Mental Illness (forthcoming May 2022) by Andrew Scull. It is a book about the history and failures of psychiatry, which probably has one of the worst track records for any science and even its apparent successes don’t seem that great in retrospect. In 1927, Julius Wagner-Jauregg won the Nobel Prize in Medicine for inoculating syphilis patients with malaria. In 1949, Egas Moniz, the pioneer of frontal lobotomies, became psychiatry’s second Nobel Laureate.
The situation often doesn’t seem much less abysmal nowadays. The dominant paradigm seems to be that there is something wrong in people’s brains and that inborn disease can be cured - to the delight of the pharma industry - with a lot of medication. The most common mental health problems are now anxiety, depression and ADHD. With one in five high school boys and one in 11 girls now diagnosed with ADHD, the United States, for example, accounts for about 92% of worldwide expenditures for treatment drugs. Anti-depressants and SSRIs are ubiquitous. Did we miss the big picture? If psychiatry is to survive, Scull concludes, psychiatrists must come up with a new paradigm.
Why isn’t the current paradigm working? Mental health problems run in families, they are inherited, some of them up to 80%. Bipolar disorder is frequently inherited, with genetic factors accounting for approximately 80% of the cause of the condition. Bipolar disorder is the most likely psychiatric disorder to be passed down from the family. If one parent has bipolar disorder, there's a 10% chance that their child will develop the illness.
However, it is when we turn to genetics that things start to get really messy. If once we were hoping to find genes and harmful mutations for psychiatric disorders, such hopes have turned out more than overly optimistic. Not that no genes could be found, on the contrary dozens and dozens of these genes have been found, but that did precious little to come up with solutions. Most of those gene variants are ancient, not recent harmful mutations. What’s more, they are interrelated. Anxiety and depression have extremely high correlations with each other as well as to the majority of mental health problems and neurodiversity (ADHD, ASD).
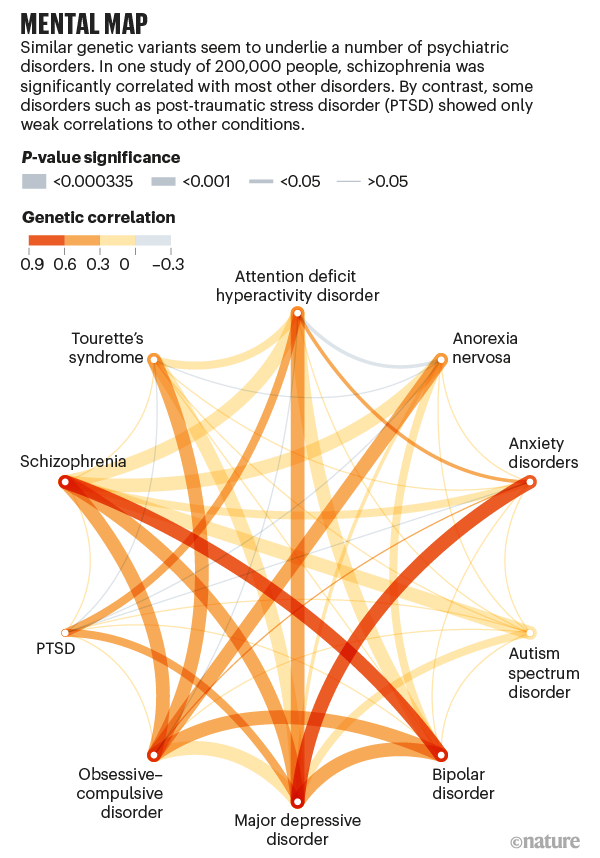
The link between neurodiversity (ASD, ADHD, gifted) with mental health problems is particularly deep, with anxiety and depression very common in neurodiverse people and bipolar disorder, very common in gifted people.
From the point of view of evolutionary psychology we have a paradox here: if these ancient genes for mental disorders are deleterious (and they most often are), why hasn’t natural selection weeded them out? Some evolutionary psychologists have proposed selective benefits for people with mental disorders, such as accompanying higher sociosexuality. This may work in individual cases for passing on one’s genes, however, it should be clear that people with such disorders have a lower-than-average chance of producing viable offspring (evolution isn’t interested in children, it’s grandchildren).
On the contrary, mental health problems have been on the increase, just like neurodiversity. One of the most interesting links is certainly mental health and creativity: autism is common in families of engineers and scientists, schizophrenia in families of artists, and there are links between high creativity with ADHD and high intelligence with bipolar disorder. There is even assortative mating among people with mental diseases. What are they selecting? It’s unlikely they desire an unhealthy person when it’s a strong and healthy personality they would need most. It has even been suggested that autism is the next step in human evolution in order to solve the new and upcoming problems humanity is facing (well, unfortunately, this is just not how evolution works).
What if psychiatry got its most basic assumption wrong? What if there is nothing wrong inside the brain of its patients? Medication mitigates the symptoms but doesn’t solve anything, after all. A new paradigm could be based on - surprise, surprise - personality. What has personality got to do with mental health? Quite a lot. To begin with, it’s known that the Big 5 factor neuroticism is highly correlated with mental health problems (after all, it’s also called emotional instability) and there is a strong link between trait openness and schizophrenia.
These correlations are only the beginning. Recently there has been increased interest in Elaine Aron’s concept of the highly sensitive person (HSP) and sensory processing sensibility (SPS). Aron claims that about 20% of people are HSPs but make up the majority of people in psychotherapy. Interestingly, Aron denies that there is a link between HSPs and neurodiversity, despite many people on the spectrum claiming they have the very same traits that Aron discovered for HSPs, sensory sensitivity first of all. Susan Cain writes in her most recent book that people with a melancholic temperament are likely to be HSPs, highly creative, and prone to anxiety and depression. Melancholic mood disorders are often accompanied by psychotic episodes.
To sum up, what we get is that about 20% of the population has a higher risk of mental disorder and there is considerable overlap between various phenomena such as HSPs, neurodiverse people (also estimated to be around 20%) and certain personality traits such as openness and neuroticism and temperament. Such differences in temperament can be observed from an early age on: children with a high reactive temperament tend to be HSPs/neurodiverse and have a detached, slow to warm up personality, i.e. they tend to observe and reflect before they act and speak and be overcontrolled (in AHDH it may be a mix between undercontrolled and overcontrolled).
Here is my hypothesis of where the temperaments come from in our evolution based on different modes of subsistence:
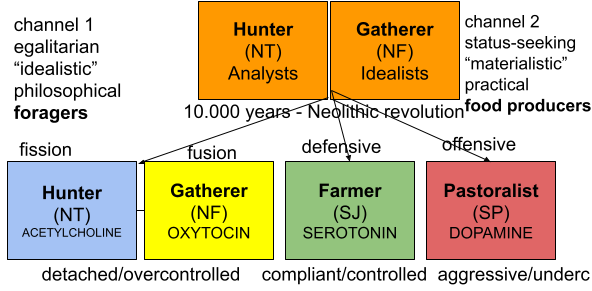
Our modern world is very much a farmer world, i.e. a world which farmer types are best adapted to: sedentary, hierarchically organised, repetitive-routine work, obedience to authority, high level of conformity, etc.
In this paradigm gatherer (prosocial forager profile) would have the highest risk of mental health problems, especially depression, anxiety and schizophrenia. Hunter types (provisioning forager profile) would be particularly prone to ASD and to some extent to antisocial personality disorder (ADPD). Pastoralist types would also have a higher rate of mental health problems, especially depression in the female caregiving profile and ASPD in the provisioning male profile.
For more on this possibly new paradigm check out my books:
Ancient genes, modern environments and mental health

The hunter-gatherer neurotribe: gifted, geeks, aspies and other aliens in this world

Comments
Post a Comment